
Keep Learning and Exploring more➡️ https://otpthealthcarerehab.blogspot.com
Low back pain (LBP) is defined as pain, muscular tension or stiffness that is localized between the costal margins and the inferior gluteal folds, with or without leg pain (i.e sciatica). An estimated 65% to 80% of population experiences LBP during their lifetime.
The prevalence of LBP increases with age and is more common in females. Certain factors like poor education, lack of exercises, low socioeconomic status, previous history of LBP, various physical factors such as lifting heavy loads, repetitive job, prolonged static posture and awkward posture have been associated with LBP. Psychological factors such as depression, anxiety, job dissatisfaction, longer working hours and obesity are also associated with LBP.
LBP can be acute (few days to 4 weeks), subacute (4 weeks to 12 weeks) or chronic (12 weeks and longer) condition.
CAUSES OF LBP :
A) Mechanical causes (triggered by spinal movement and involves spinal structures) includes :
- Abnormal curvature (scoliosis, khyphosis, lordosis)
- Degenerative disc, prolapsed intervertebral disc
- Ligament sprains
- Muscle strain
- Pinched nerve (sciatica or lumbar radiculopathy)
- Spondylolisthesis
- Spinal stenosis
B) Organic causes ( due to disease, connective tissue disorder) includes :
- Benign or cancerous spinal tumors
- Cauda equina syndrome
- Osteoporosis
- Osteoarthritis
- Osteomyelitis.
- Fibromyalgia
- Ankylosing Spondylitis
- Rheumatoid arthritis
SUPPORTING STRUCTURES OF SPINE
These can be divided into skeletal and muscular systems. Both systems are essential to support spine during static and dynamic postures. It is essential for therapist to have knowledge of specific or target spine muscles for rehabilitation.
In this article we will focus on muscular supporting system of spine. This system can be divided into inert supporting structures and muscular supporting structures.
A) Inert structures (can also be considered as static stabilizers of spine) : Static stabilizers are the non-contractile tissue of the joint. They are very important in spine stability at end-range ROM and/or when there is a dysfunction of the dynamic stabilizers. Joint capsule and ligaments provides passive resistance to motion. In spine, ligaments are slack in midrange and taut at end range when a structure limits movements in a specific directions and thus provides stability in that direction.
Various inert structures are:
- Forward bending is limited by interspinous and supraspinous ligament, capsular ligament, ligamentum flavum and posterior longitudinal ligament.
- Backward bending is limited by anterior longitudinal ligament.
- Side bending is limited by contralateral intertransverse ligament, ligamentum flavum and capsular ligament.
- Rotation limited by capsular ligament.
- Intervertebral discs : it is a shock-absorbing structure between each vertebra. The disc has thick outer layer (annulus fibrosus) that surrounds the soft gel-like center (nucleus). Annulus fibrosus is organized in concentric rings. Some fibers are taut in whichever direction the spinal segment rotates or sheers. Fibers slack on side of concavity and taut on side of convexity. Features of intervertebral disc is that greater the ratio of disc thickness to vertebral height the greater the mobility.

Fig 1 : Inert supporting structures of spine
B) Muscle structure (also called as dynamic stabilizers) : Dynamic stabilizers is defined as muscles whose isometric or stabilizing contractions maintains control of the functional position in response to imposed fluctuating forces through the moving extremities. Muscular structures of trunk not only acts as a prime movers or as antagonist to movement caused by gravity during dynamic activity, but also provide stability of spine. These muscles crossing the joint is responsible for keeping the opposing joint surfaces in proper alignment for efficient joint mechanics while performing any manual activity.
They are divided into 2 types :
- Global muscles : these are superficial (further from axis of motion). These muscles re unable to stabilize individual spinal segments as they have no direct attachment to the vertebra. They provide compressive loading with strong muscle contractions. Ex: Rectus abdominis, External and internal Obliques, Quadratus lumborum (lateral portion), Erector spinae (medially Spinalis, centrally Longissimus, laterally Iliocostalis), Iliopsoas.
- Deep / segmental muscles : they have direct attachment across vertebral segments. They maintain each segment in a stable position and provide dynamic support to each segment. Thus, decreasing the stress on inert tissues at the limits of motion. Ex: Transverse abdominis, Multifidus, Quadratus lumborum (deep portion), deep rotators.
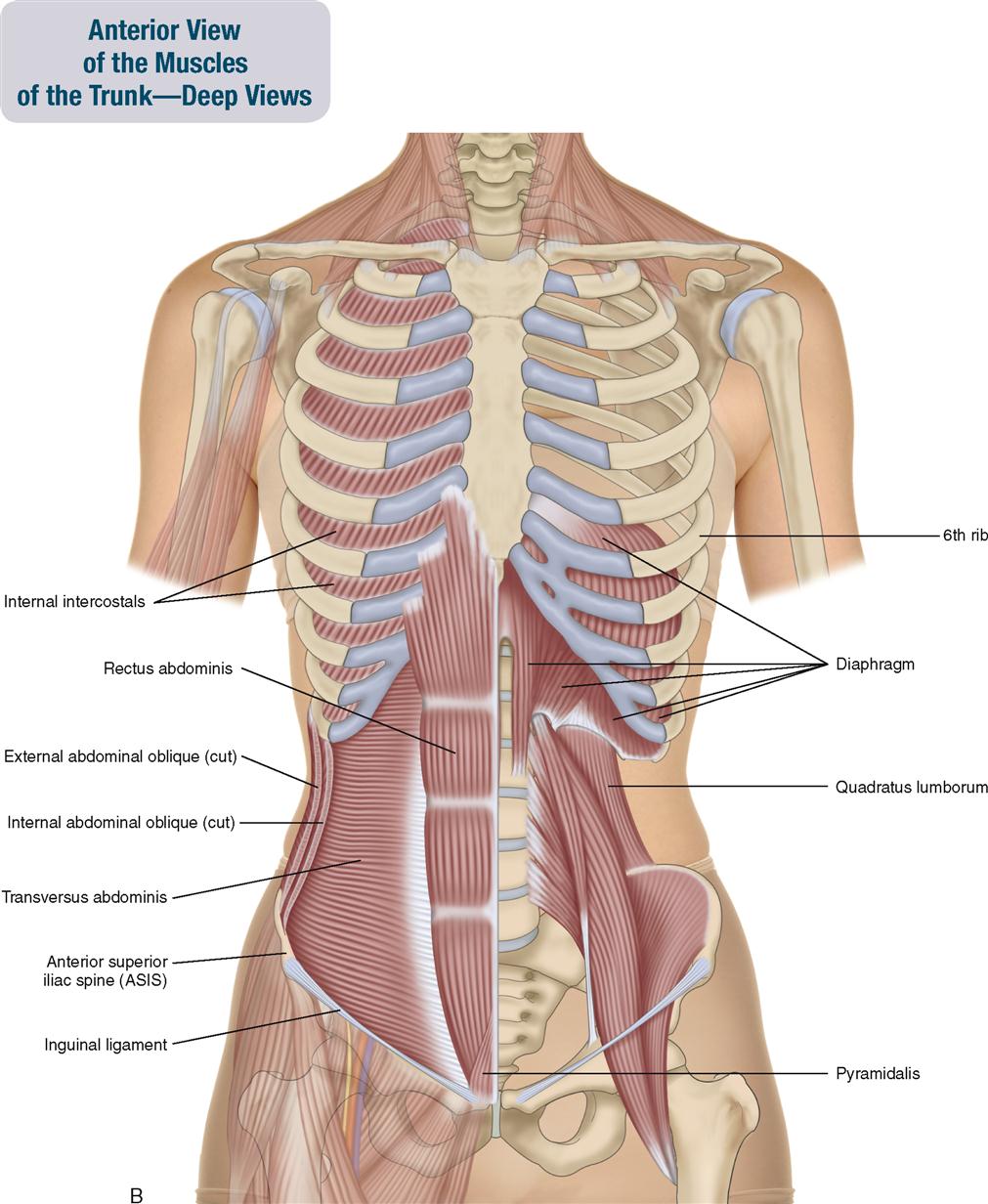
Fig 2 : Anterior view of spinal muscular structure
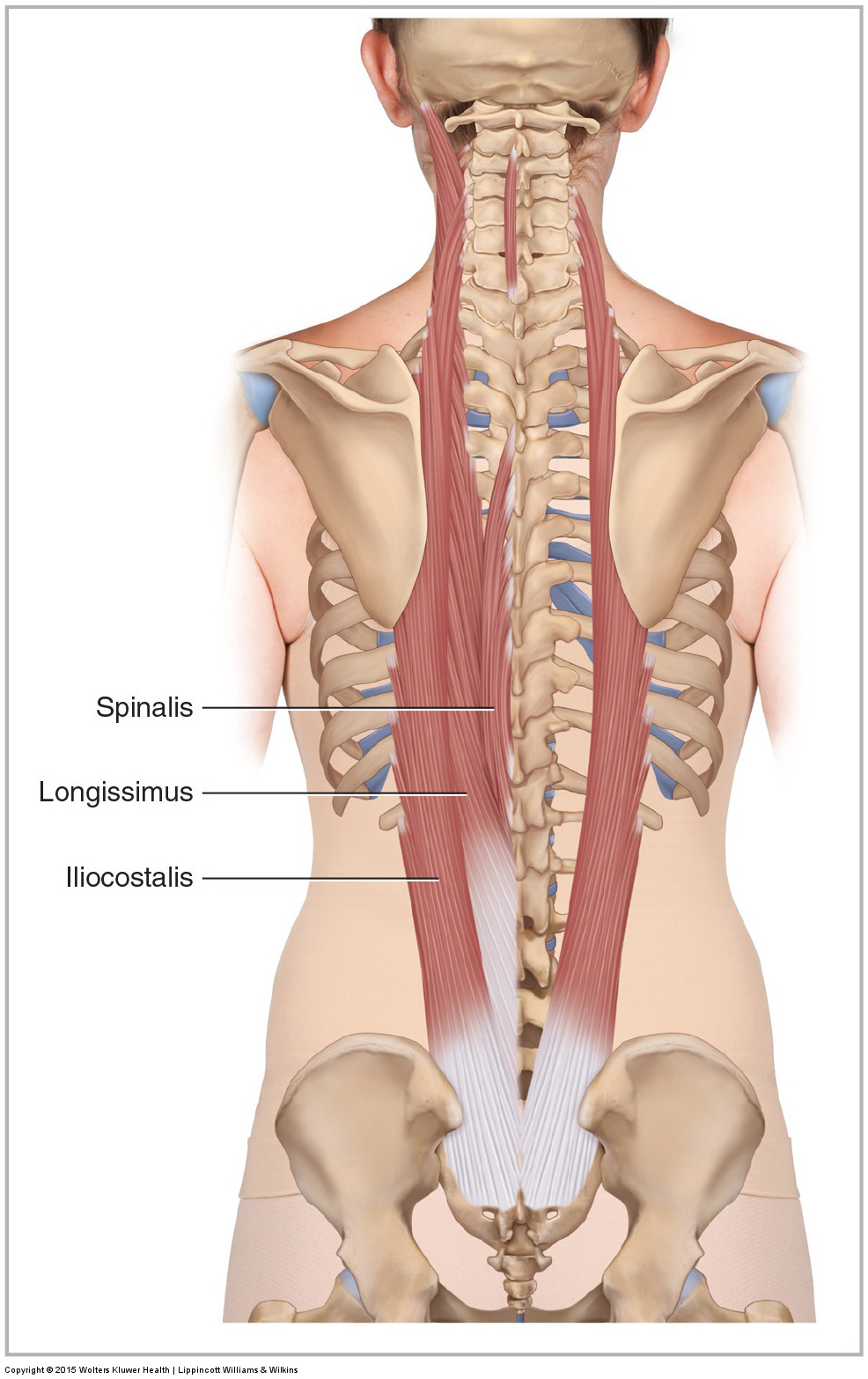
Fig 3 : Erector Spinae muscles (Global muscle)

Fig 4 : Multifidus muscle (deep structure)
Thankyou for reading!!!
( Dr.Ashwini Sangar, Dr. Sheetal Tatar-Dhande, Dr. Pallavi Khadse-Kolhe)
Comments