
Keep Learning and Exploring more➡️ https://otpthealthcarerehab.blogspot.com
INTRODUCTION
- Extradural e.g. leukaemic deposits, bony tumor, nerve sheath tumor
- Extramedullary-intradural e.g. meningioma, neurofibroma,
- Intramedullary-Intradural e.g. ependymoma, astrocytoma, hemangioblastoma
- Infections (peripheral nerve affected): Guillain Barre Syndrome (GBS), Poliomyelitis or Postpolio syndrome
- Hereditary: Hereditary Spastic paraplegia, Spinal muscular atrophy,
- Muscular dystrophy: Duchenne muscular dystrophy, Becker's muscular dystrophy, Limb-girdle muscular dystrophy
Causes of Cerebral Paraplegia:
1. Causes in the Parasagittal Region: (area of cortical presentation of L.L.) it includes
· Traumatic e.g. depressed fracture of the vault of the skull, Subdural haematoma.
· Vascular e.g. superior sagittal sinus thrombosis.
· Inflammatory e.g. encephalitis, meningio-encephalitis.
· Neoplastic e.g. parasagittal meningioma.
· Degenerative e.g. cerebral palsy.
2. Causes in the Brain Stem:
Syringobulbia and midline tumors. These lesions arise in the midline and
involve the innermost fibers which are those of the lower limbs.

PATHOLOGY OF SPINAL CORD NEURAL INJURY
The displaced vertebra may either damage cord, cord along with the nerve roots or the root alone. Damage to neural structures may be:
1] Cord concussion:
- disturbance in functional loss without a demonstrable anatomical lesion.
- motor paralysis(flaccid), sensory loss and visceral paralysis occur below lesion.
- recovery begin within 8 hours, and eventually the patient recovers fully.
- cord and surrounding tissue transected.
- injury is irreparable and anatomical lesion present.
- flaccid paralysis(acute) ----’spinal shock’(24 hours to 6 weeks )----no control from higher centres---- no voluntary control, loss of sensation and autonomic functions, acts as independent structure(below lesion) ----manifest reflex activity at spinal level .
- appearance of signs suggestive of reflex cord activity: bulbocavernous sign and plantar reflex, without recovery of motor power or sensation is an indicator of cord transection.
- Stages of reflex activity:
- spinal nerve root may be damaged alone in injuries of the lumbar spine (cauda equina affected), or in addition to cord lesion, in injuries of the dorsal lumbar spine.
- residual motor paralysis is permanent and regeneration is theoretically possible.
- a discrepancy between neurological and skeletal level may occur in spinal injuries below D10 level because the root descending from the segment higher than the affected cord level may also be transected, thereby producing higher neurological level than expected.
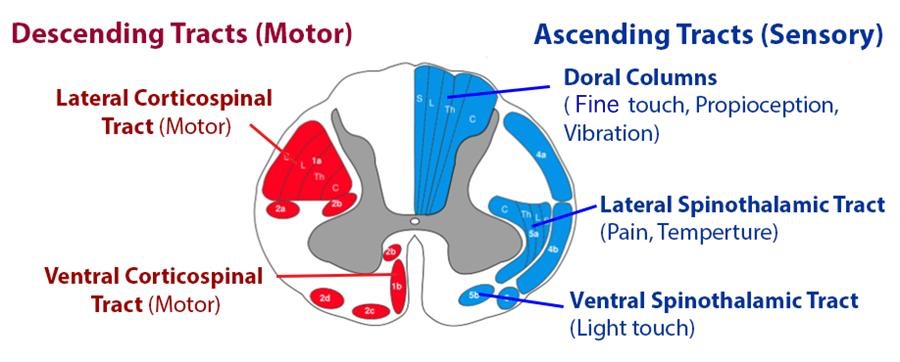
- Brown-Sequard syndrome: occur from hemisection of spinal cord and clinical features are asymmetric ----typically by penetrating wounds i.e. gunshot or stab. On ipsilateral side there is loss of sensation in dermatome segment and paralysis of lesion side, clonus, babinski sign positive. Dorsal column involved: loss of proprioception, vibratory sense and kinesthetics sense. On contralateral side there is damage to spinothalamic tracts resulting in loss of sense of pain and temperature. This loss begins several segment below the level of injury.
- Anterior cord syndrome: complete paralysis and anaesthesia present but deep pressure and position sense are retained in the lower limb (dorsal sparing) because they are mediated by posterior column with a separate vascular supply from the posterior spinal artery.----Caused due to flexion injuries of cervical spine.
- Central cord syndrome: commonest incomplete lesion. There is initial flaccid weakness followed by LMN type of paralysis of upper limbs (as cervical tracts are more centrally located) and UMN or spastic paralysis of lower limb(lumbar and sacral tracts are located more peripherally), with preservation of bladder control and perianal sensation (sacral sparing)---- hyperextension injuries of cervical spine.
- Posterior cord syndrome: it is characterised by isolated ipsilateral loss of vibratory, two point discrimination and conscious proprioceptive sensations. There is ipsilateral loss since the ascending fibers have not crossed. It is a rare condition and occurs when tha damage is towards the back of spinal cord.
- Sacral sparing: it refers to incomplete lesion in which the most centrally located sacral tracts are spared. Varying level of innervation from sacral segment remain intact. Clinical signs perianal sensation and external anal sphincter contraction.

Thankyou for reading!!!
( Dr.Ashwini Sangar, Dr. Sheetal Tatar-Dhande, Dr. Pallavi Khadse-Kolhe)
Comments